

As you may know, I have type 1 diabetes. The following posts are from my Diabetes Awareness Month series in 2017, and hopefully they give you a glimpse into my everyday life:

This pumpkin contains the 526 syringes I injected myself with during the month of October. It does not include the other 411 lancet needles I also used in October -- the pumpkin simply had no room. 937 needles in one month. It's the first time I've ever done a #T1DPumpkinPoke, but if I'd consistently done these, pumpkins just like this one would legitimately cover my entire (large) room.
If it's 8am, I need a shot. If it's 4pm, I need a shot. If it's midnight, I need a shot. Before my feet touch the floor in the morning, I need a shot. If I eat, I need a shot. If I eat just a bite of broccoli, I still need a shot. If I'm stressed, I need a shot. If I'm nervous/anxious/excited/scared, I need a shot. If I exercise, I need a shot. If I take certain other medications, I need a shot. In certain weather/altitude conditions, I need a shot. If I'm sick, I need extra shots. If it's that time of month, I need extra shots. If I don't sleep enough, I need extra shots. I think you're catching on here.
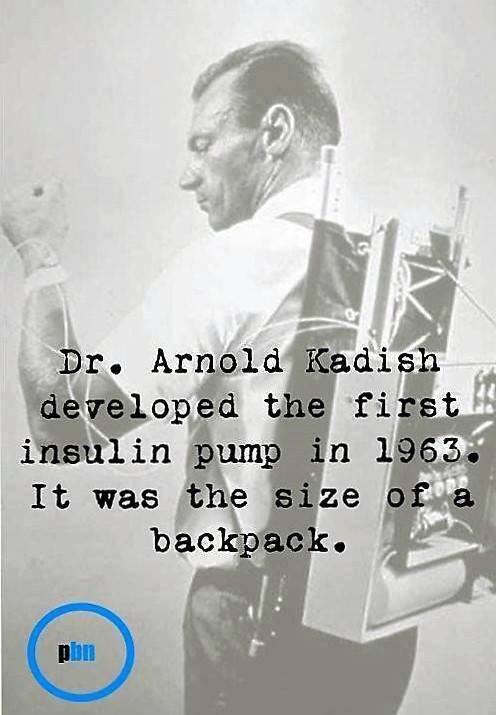
Being my own pancreas is hard work. It might surprise you that shots are the easy part of it all for me. And I'm really lucky. I have access to my medicine and can afford my medicine. I'm lucky to live in the 21st century. Before 1921, it was a death sentence globally, and sadly today, it's still often a death sentence for children in developing countries. I'm lucky to have a disposable, sharp syringe for each and every injection. My great grandfather and great aunt had to sharpen their reusable glass syringes on the stove each night. I'm lucky that I'm now 24 and the pain from syringes/lancets hasn't bothered me for years, but could you imagine having to give all of these needles to a young child (we're talking as young as ~6 months old here)?
My pancreas isn't something I talk to most people about much (or at all), even those whom I know very well, but it is definitely something I am open to talking about. Most people completely take their pancreas for granted, and of course they do, why wouldn't they? I know many feel Facebook is too crowded with awareness posts, but in my view, they're important. So, I'm going to do my part this month and help spread some awareness. If you choose to follow my posts throughout T1D awareness month, hopefully you’ll have a better understanding of what it is, what it’s like living with it, what the symptoms are (especially given my entire friend list seems to be getting engaged/almost having children), and why there are so many misconceptions.
------------
I am truly amazed by the response to my #T1DPumpkinPoke post yesterday. Never could I have anticipated over 2,300 shares and hundreds of thousands of impressions. Thanks so much to everyone who read/liked/shared my post and helped move forward this awareness initiative. I wasn't planning to post this particular follow up, but given the debate it's stirred in the T1D community, here it goes.
T1D is such an individualistic thing. It really is. What works for me may work differently for you. I mean, what worked for me yesterday may not even be what works for me today. Seriously. It's that variable.
I received 313 messages over the past day from T1s/T1 parents. The two main "questions" I received were:
1) My daughter/son only takes 8-10 injections per day...why are you taking 16? You need a new doctor. Are you crazy? You're doing this wrong. Are you making this up?
2) Why don't you just get a pump?
Here's my response. I am managing my T1D according to Dr. Bernstein's approach to optimize for health outcomes. While a few more shots a day might be a pain, the results pay off both short term and long term for my health and happiness. There is a blood test called a1c which, although is not a perfect test, is a rough reflection of how I'm doing at being a pancreas. My a1c is 5.1 and has been 5.0-5.2 for years, which is the same as the rest of my non-D family. From blood work alone, you could not tell a functioning organ from how I'm doing at being a pancreas. Let that sink in.
Bottom line is, I am extremely happy with how I manage my T1D. Period. As I said in my post, shots don't bother me, but having anything other than a non-D a1c WOULD bother me. I will not judge/criticize/evaluate your approach -- that's none of my business. If you are happy with a different approach, great, I'm glad it's working out for you!
To answer the second question, I was on a pump for 8 years. And 8 years of personal experience is enough to know what's best for me. Yes, I've tried Omnipod, TSlim, Medtronic, APS, you name it. I will share more about my pumping experience in future posts, but long story short, it IS possible for ME to achieve better outcomes on MDI than pumping AND be much happier. You might have a completely different experience. And that's entirely okay.
Now back to my planned #T1DAwarenessMonth programming.
------------
I live an incredibly normal, fulfilling and happy life with T1D. In fact, I think that’s one of the reasons many friends were so surprised by my #T1DPumpkinPoke post, as unless I told you, you’d have no clue. It really hasn’t stopped me from doing anything. I went to college 1,218 miles from home, lived alone for 4 years, traveled abroad for 2 semesters and have worked at Google for the past 2.5 years. While I will cover the hard parts of T1D because I want my posts to be as accurate and realistic as possible, the positives of T1D are certainly a necessity in providing you a comprehensive picture. To be clear, of course I’d rather not have T1D, but it has changed my life for the better in countless ways. It really has.
First and foremost, it’s taught me that everyone has their challenges, health-related or not, many of which are invisible. T1D has given me a strong sense of empathy and ability to give people the benefit of the doubt. You have absolutely no clue what someone else is going through.
I've been 100% independent in managing my T1D since age 14. Commonly, parents are still very involved in T1D management (especially overnight care) until age 18, or even beyond. It therefore gave me incredible maturity from a very young age. I am responsible in every aspect of my life, and T1 largely deserves the credit.
T1 has given me a unique sense of appreciation for each day. Waking up is a beautiful thing when you’re responsible for your own survival. I mentioned this in my original post, but I have a lot to be thankful for in this respect.
Some things are within my control, and some things are not. T1 has its ups and downs, and life has its ups and downs. I've had enough truly bad days to know that 99.9% of days are actually great days. I influence what I can, face adversity with resilience and truly don't "sweat the small stuff," as cliche as it sounds.
My impeccable organization and planning ahead skills stem from T1. In my personal and professional life, I literally calendar every single minute of my day — even if it’s in 5 minute time chunks. I can almost guarantee I wouldn’t be as effective at this without T1D.
I am always thinking about the future consequences of my current actions. How I manage my T1 now WILL matter greatly down the road. Planning ahead and mapping out my future has proven to be a great life skill that T1 taught me first.
I am incredibly in-tune with my body because of T1 and am extremely proactive with my health. I'm thankful that T1 has prompted me to make good decisions for my overall well-being.
T1 taught me the power of connecting with like-minded people. The bond I have with other T1s is hard to describe. They just know and understand me in a way no one else ever could, even my closest friends and family. While I’m also a firm believer in diversity of experience, these connections have proven to be of the “1 + 1 = 3” sort.
Finally, T1D has taught me about pride and celebrating your own successes. Less than 1% of T1Ds* are achieving the a1c results I’m achieving, and that’s something to be proud of.
*Source: T1DExchange, https://t1dexchange.org/pag…/resources/our-data/t1d-discover
------------
I mentioned in my #T1DPumpkinPoke post that all of the needles are not the hard part. What's the hard part?
The hard part is having something so consuming to you that is entirely invisible to the rest of the world.
The hard part is facing the reality that the same medicine that saves my life everyday is lethal with the slightest imprecision in dosing.
The hard part is knowing that very few people know how to use my life-saving emergency injection if I'm found unconscious.
The hard part is feeling uncomfortable in social/business/dating situations when I find it more challenging to do what I need to do for my health.
The hard part is how much mental energy it takes to be a pancreas. Calculations are always running through my head. With almost every other disease, your physician can tell you how much medicine you need. With T1D, they can give general recommendations, but depending on dozens of factors the amount of medication you need changes.
The hard part is never having a break. There is no one else who can provide relief, not even for a minute. Birthdays, holidays, vacations, you name it. And being my pancreas overnight. T1D never sleeps, and my sleep is therefore disturbed quite frequently.
The hard part is trying not to let T1D change decisions I make and parts of my personality, but knowing it has.
The hard part is having to always plan ahead. Spontaneity just doesn't work with T1D.
The hard part is having to rely on imperfect technology. I was severely affected by an FDA recall a little over four years ago and not a day has gone by that I haven’t wondered how things might have been.
The hard part is when I'm alone and emergencies arise - like the time I regained consciousness on my bathroom floor and still don't know how I got there or what happened beforehand.
The hard part is losing T1D community members to T1, like my friend Mandy who passed away in March, far, far too young. I think about her regularly, and it hurts. Badly.
The hard part is seeing all of the struggles T1 parents share about their baby and toddler T1s.
The hard part is having a body entirely covered in scar tissue from thousands and thousands of injections.
The hard part is worrying that my future children, nieces and nephews have a slightly higher than average risk of getting T1.
The hard part is having several other autoimmunes and health conditions that aggravate T1. As if T1 wasn't hard enough.
The hardest part is knowing that there is no end in sight. I never even let myself think about what life might be like post-cure.
------------
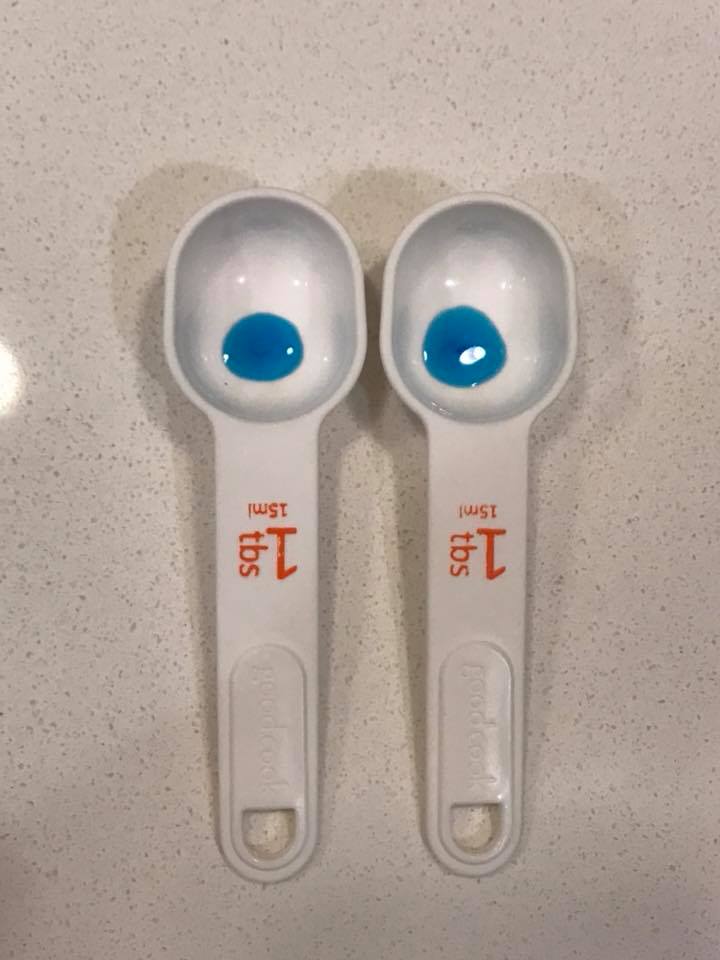
I want to go into a little more detail about one of the items from my post yesterday. In this picture you see two tablespoons. On the left is the average amount of medicine I need each day to stay alive, which I spread out into about 15 shots. The extra “drop” I put into the right tablespoon would kill me, likely within about 2 hours. Yes, the difference is a tiny, tiny amount.
Remember, *I* am the one deciding how much to take. If my doctor could just tell me the exact amount of medication I needed, it would be easy. I could just draw up the proper amount, double check it for accuracy, and be on my way. The truth is, every dose is an educated guess. And that's a scary thought when your own life depends on your educated guess. In a hospital setting, 2 medical professionals must validate the dose before giving it to any patient. And yet, T1s must decide this for themselves multiple times a day. Dosing the perfect amount is hard. Extremely hard. I’m oversimplifying things here, but essentially, giving too much is typically dangerous immediately and not giving enough is typically dangerous long term. Doses both too small and too large have short term side effects too, sometimes which are quite extreme.
Sometimes I have the luxury of planning out my dosing. I factor in when I'll be eating, what I'll be eating, how much activity I'm expecting, how much sleep I got, how stressed I am, what part of my cycle I'm in, etc. While I tend to achieve better outcomes in these situations, that's not always the case. Even if I try to keep all variables the same, my needs can fluctuate day-to-day. Other times I'm making these decisions completely on the fly. At 2 a.m. when I'm half asleep. In the middle of a first date when I have a quick moment to sneak in a shot. At a red light. During a meeting. At a new restaurant when I really have no idea when the food will arrive, how big the serving will be, etc.
Wrong educated guesses happen. It's the reality of life with T1D. The method I use to manage my T1D minimizes the overall amount of medication I need. This is a great thing because of "the law of small numbers." Smaller doses minimize the effect of dosing errors. The most important part is quickly identifying the error in either direction and treating it promptly -- even if that means another shot.
P.S. No, my medication is not blue. But blue sure does generate quite a bit more attention than clear.
------------
“It could be so much worse. At least you have T1D and not cancer.”
I hear this all of the time. From personal experience I’m 100% aware that there are worse health conditions than T1D, but statements like this undermine the hard reality T1s face everyday. Of course I’d rather have T1 than cancer. But when would an individual get to choose between T1 and cancer? Um, never! Comparisons among diseases need to stop, especially among individuals who have neither. (If you have both, compare away if you so choose.)
T1 is not something anyone ever asked for, and there is no way to prevent it. It is an autoimmune disease where the body’s own immune system kills the pancreas’ beta cells. In fact, they still don’t even know for sure what causes it, but likely a combination of genetic and environmental factors. T1 happens to run in my family, but many who are diagnosed with T1 have no family history. It has nothing to do with poor diet, lack of exercise and obesity. Babies who have consumed nothing but breast milk get diagnosed with T1D even.
T1s only account for 5-10% of all diabetics. Type 2 diabetes is an entirely different disease - one of insulin resistance versus no insulin production. Given the prevalence of type 2 in the media, it’s become nearly synonymous with diabetes to the average person, further placing type 1 under the radar. While T2 can sometimes be reversed or improved, T1 is irreversible, and kids never "outgrow" T1.
It’s national diabetes month, so even though all of my other posts focus on T1, I want to share a brief comment on type 2. Guess what, no one with type 2 diabetes wanted a disease either. Type 2s face a ridiculous amount of blaming and shaming. That isn’t helpful. It really isn’t. Given type 2 does have clear risk factors and some prevention measures that can be taken, I of course do believe initiatives to prevent type 2 are beneficial, but type 2 diabetes is nothing to joke about.
Diabetes is the only disease I can think of that is so commonly used in jokes, and there’s nothing funny about it. In fact, diabetes jokes are flat out damaging, especially to T1 kids. They make them feel ashamed and embarrassed about their disease, when neither they nor their parents did anything wrong. And the stereotypes that diabetes jokes perpetuate make it much, much harder to tell people you have T1D. There’s a super slim chance they’re familiar with T1, and telling someone you have diabetes commonly results in an instant judgement, even if they have the best intentions. Trust me on this one.
So, in short, my ask this #T1DAwarenessMonth is that we all take an extra moment to think before talking about illness. Is what you have to say harmful? Unhelpful? Perpetuating false stereotypes? Unkind? If so, please think again.
------------

The cost of T1D isn't something I've covered in my posts yet, largely because I'm really fortunate that it isn't one of the first things I have to think about when I think of T1D. But in this picture, you see the T1D prescriptions I fill on a monthly basis. $2,307.83 total per month, and that doesn't include several other non-prescription T1D expenses like alcohol swabs, gauze, sharps boxes, etc. There are also annual costs not pictured here that add up to well over $1,000.
If you do the math, that's $29,187.13 in T1D prescriptions alone a year. And I'm not even on the pump, which can add thousands more. Fortunately, insurance does cover quite a bit of this expense for me, but keep in mind, not everyone with T1D has great insurance, or insurance at all.
Accessing and affording T1D supplies is an extremely serious problem for hundreds of thousands of the 40 million people around the world with T1D. There's an organization I've been volunteering for, T1International, that tackles this problem head on. I'm very proud of the work they do. In short, they support and empower local communities and equip them with the tools they need to make progress on this issue. Specifically, I bring my background in digital marketing to help T1International distribute its Advocacy Toolkit, achieve greater awareness of the T1D landscape and acquire new advocates and donors.
In Zambia, T1D supplies commonly cost TWICE a family's income. In many other countries, T1D can cost as much as 75% of a family's income. If you're interested in learning more about how T1D supply access and affordability varies around the world, check out T1Internationals's Global T1 Map Tool: https://www.t1international.com/map/
------------
For today’s #T1DAwarenessMonth post, I’m sharing a well-written T1D symptom awareness post by my friend Alison: “Did you know that anyone at any age can be diagnosed with type one diabetes? Davin was just 8 months old when he woke one dreary day in April and began screaming, vomiting and became very lethargic. I hadn't noticed any other symptoms he had been displaying for a couple weeks prior. The only strange thing was he was going through diapers like crazy. I honestly thought we had bought a defective package of pampers. I rushed Davin to the Dr that day. He was diagnosed with Type One Diabetes and he was in Diabetic Keto Acidosis. We was so sick, we could have lost him had I not brought him to the dr and I'm thankful his pediatrician decided to run a blood glucose test. I have no pictures from that dreadful day. The memory is enough. I'm sharing a picture of Davin (in the basket) just a week before his diagnosis and also a picture of him a few months after his diagnosis sporting his insulin pump and a great big smile. Please know the symptoms of T1D. It may save a life.”

------------

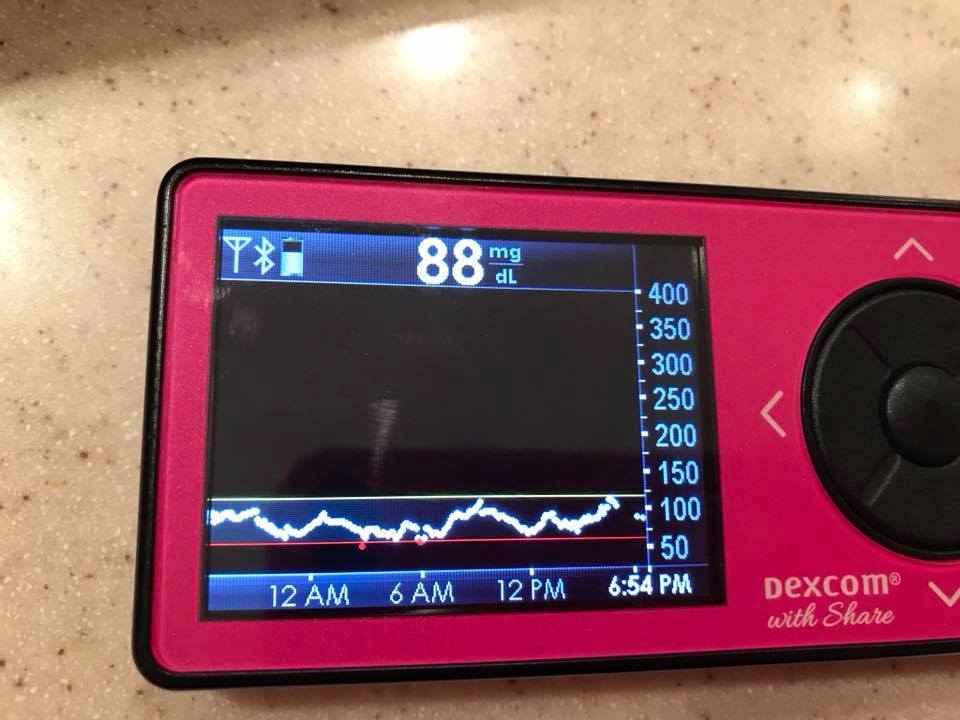
For today's #T1DAwarenessMonth post, I'll be covering CGMs (continuous glucose monitors), which I'd argue is the best technology available for T1Ds. CGMs give a new reading every 5 minutes. For parents with T1s who are too young to talk/express how they feel, CGMs are truly life-changing. For me personally, it's helpful with overnight monitoring and knowing exactly when I need to give a shot. It is also reassuring to see how I'm trending.
I've owned a CGM since 2008, though I haven't worn it consistently. When I first got one, it was a very clunky device and the accuracy was pretty poor so false scares were quite common. It's amazing to see how far CGM technology has come in just 9 years. Today CGMs have much better accuracy and the insertion is less painful. They also allow for remote monitoring, meaning others can view the real-time data from their phones when they are not with the T1 in person. This is a game changer particularly for parents while their kids are at school, as I'm sure you can imagine T1D is a lot for schools to handle.
My CGM alarms when I need to take action, or when things are progressing towards a potentially dangerous situation. I do my best to preempt the alarms by taking action beforehand. Though it's an incredible tool, it's still not perfect. Inaccurate readings can happen, especially if you put pressure on it, and heat can alter readings as well. I always like to confirm its reading before I inject to prevent me factoring inaccurate information into an important dosing decision. Unfortunately I also have a tape allergy (any and all tapes -- I've tried 25+ brands/related products), so CGMs are quite uncomfortable for me to wear and I develop serious rashes. I therefore commonly take CGM breaks, even though I really do value CGMs. And I will say, it feels amazzzzzzinggg to have nothing attached to me.
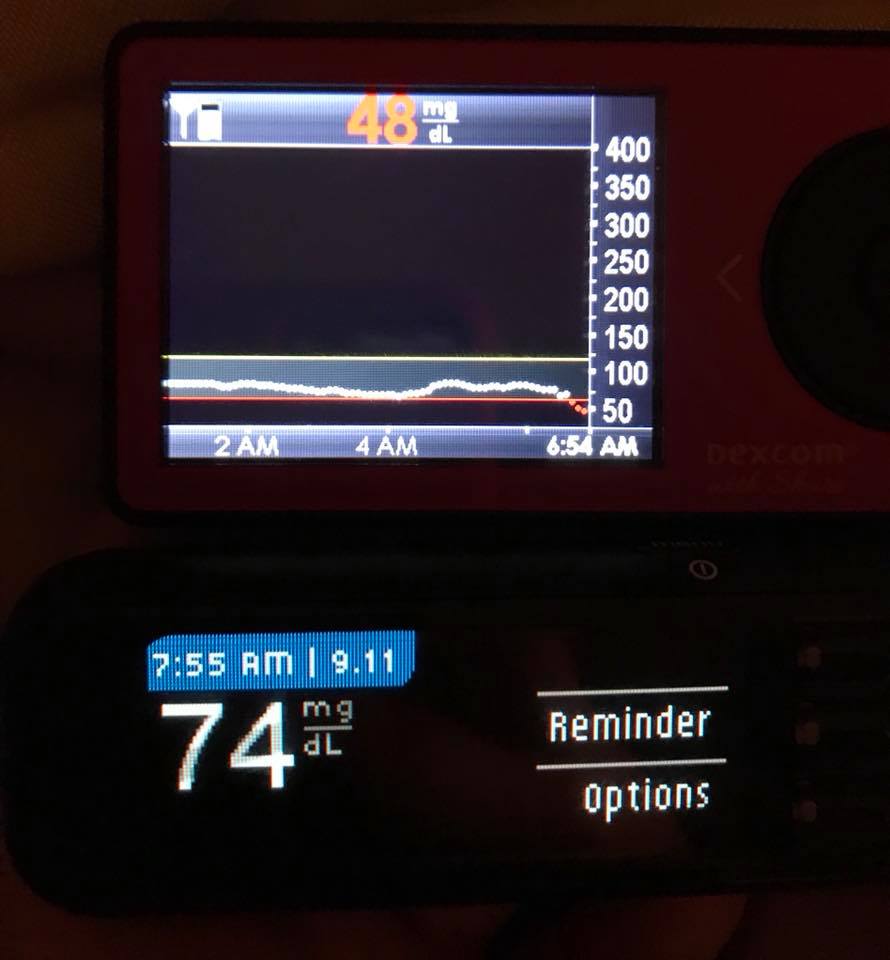
I try to stay within the lines at all times because that's the results a functioning pancreas would deliver. This, of course, is not always possible. If I dose too much or too little because I'm a human and not a pancreas, that's when I go outside of the lines. This also happens commonly when unexpected emotions/stress/hormones/illness/activity affect my graph. That said, if my graph is relatively flat and in range, I'm happy. The graph pictured is my last 24 hours, which looks like a pretty typical day for me. It consisted of 14 shots, 11 lancets and one false low alarm, where you can see I verified it against my meter. This illustrates why I verify the accuracy before assuming I’m just 48 - there’s a BIG difference between what I’d do at 48 versus 74, where I don’t need to do anything. I commonly correct highs at 100 but have my top line set at 120, as Dexcom will not allow it to go lower. The bottom line is set at 65. I feel great 60-90, though prefer to be in the 80s in a perfect world.
------------
------------


Today's #T1DAwarenessMonth post is on T1D and extreme fitness. I went to an event today called Bolus & Barbells, which essentially is an event for hardcore athletes with T1D. I am definitely not a serious athlete (or an athlete at that!), but given people traveled from all over the world for this and it was held at a CrossFit gym just minutes away for me, I decided to register.
I was particularly inspired by Kyle Cochran, a T1 American Ninja Warrior Finalist. He was diagnosed with T1D when he was 5 years old. He shared quite a few funny stories, including one where he gave himself an injection for Kindergarten Show & Tell and 2 kids passed out and 1 threw up. He explained that he is grateful for T1D because the harder the obstacle, the stronger you get. During American Ninja Warrior season, he trains FOUR HOURS everyday. His body fat percentage was even too low to wear a continuous glucose monitor (CGM). Clearly, extreme sport is possible with T1D, though it certainly comes with its own challenges.
I've shared some pictures and videos from the event. You can see Kyle doing push ups with no feet and another T1D pulling a Jeep. Amazing stuff!
------------

Today's #T1DAwarenessMonth post is on #DiabeticAlertDogs. This is me with Grus, my friend Hillary’s amazing and adorable diabetic alert dog (DAD). DADs are truly incredible. Through scent, they can detect when blood glucose is out of range and alert their humans. The exact alert mechanism varies based on their training, but one paw for lows and two paws for highs seems to be common. In this regard, they perform a similar function to CGMs, except often with much better accuracy.
But that's where the similarities end. DADs can actually help out T1Ds by assisting in treating these situations. For example, they can be trained to bring meters or hypoglycemia supplies to their humans. For kids with DADs, they can also get their parents in order to help them help their T1.
I know several T1s with DADs, many of which are as young as 3 years old. Oftentimes, DADs are in addition to CGMs versus instead of since both have unique advantages. Certain breeds work better for becoming DADs, but even my 6-pound malshi has 100% success rate in waking me up for low blood sugars overnight (that is when I let her sleep in my bed, as those of you who know me well know that's a pretty rare occurrence since I’m not much of a dog person). Pretty amazing that dogs are so perceptive to glucose fluctuations!
------------
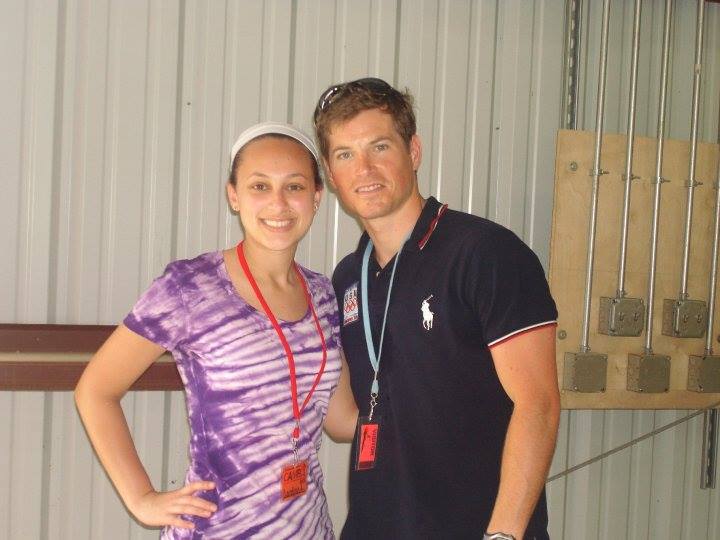
Today's #T1DAwarenessMonth post is on famous people with #T1D. This is a picture of me and Kris Freeman, a U.S. Olympian skier (it's 8 years old, but still my only picture with any famous T1). So who else has T1D?
Nick Jonas
Bret Michaels
Sonia Sotomayor
Elliott Yamin
Crystal Bowersox
Jay Cutler
Sharon Stone
Theresa May
Nicole Johnson (Miss America)
Usher's son
....and so many more!
------------
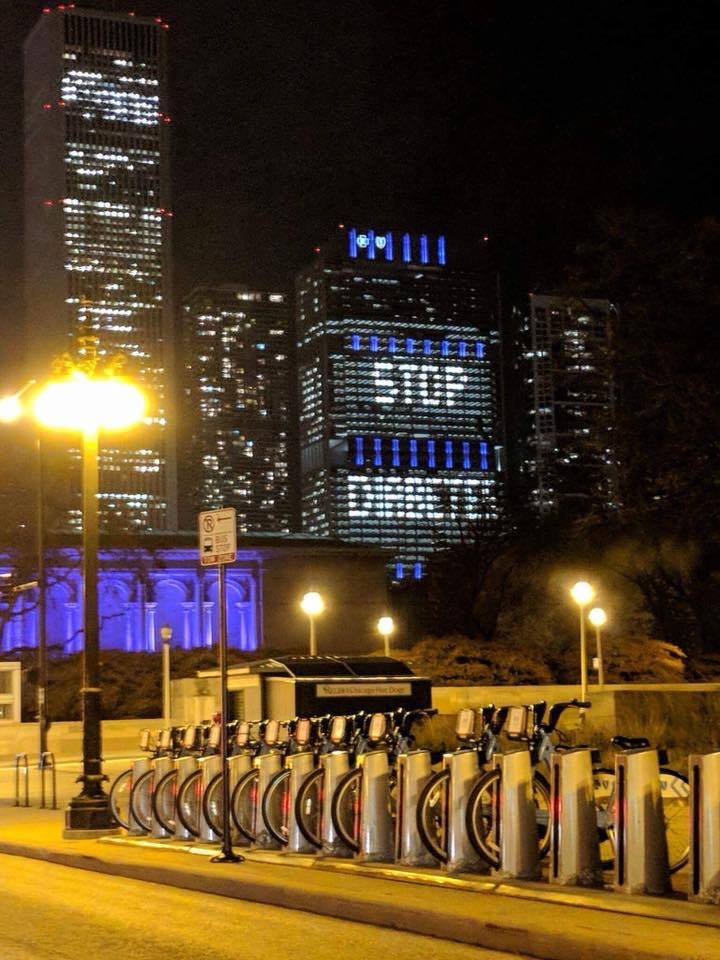
Today is #WorldDiabetesDay in honor of Dr. Frederick Banting's birthday, the physician that discovered the hormone insulin in 1921. World Diabetes Day encompasses both type 1 and type 2 diabetes. Over 1,100 buildings worldwide today "went blue." Check out this building in Chicago! Its verbiage "Stop Diabetes" isn't super type 1 friendly since type 1 cannot be prevented, but it still raises awareness in a beautiful way!
------------

Today's #T1DAwarenessMonth post illustrates the discovery of insulin:
"In 1922, scientists went to a hospital ward with T1D children, most of them comatose and dying. This is known as one of medicine's most incredible moments. Imagine a room full of parents sitting at the bedside waiting for the inevitable death of their child. The scientists went from bed to bed and injected the children with the new purified extract - insulin. As they began to inject the last comatose child, the first child injected began to awaken. Then one by one, all the children awoke from their comas. A room of death and gloom became a place of joy and hope."
It's absolutely mind-boggling that this was less than 100 years ago! While I'm incredibly grateful for insulin each and every day, it's important to note that insulin is NOT a cure for T1D -- it's life support.
------------
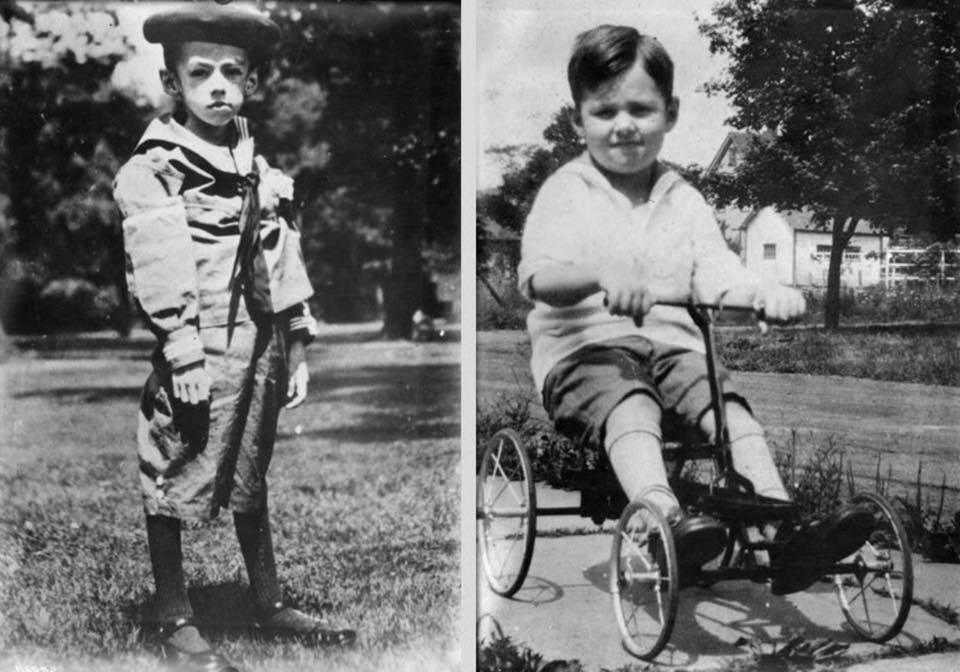
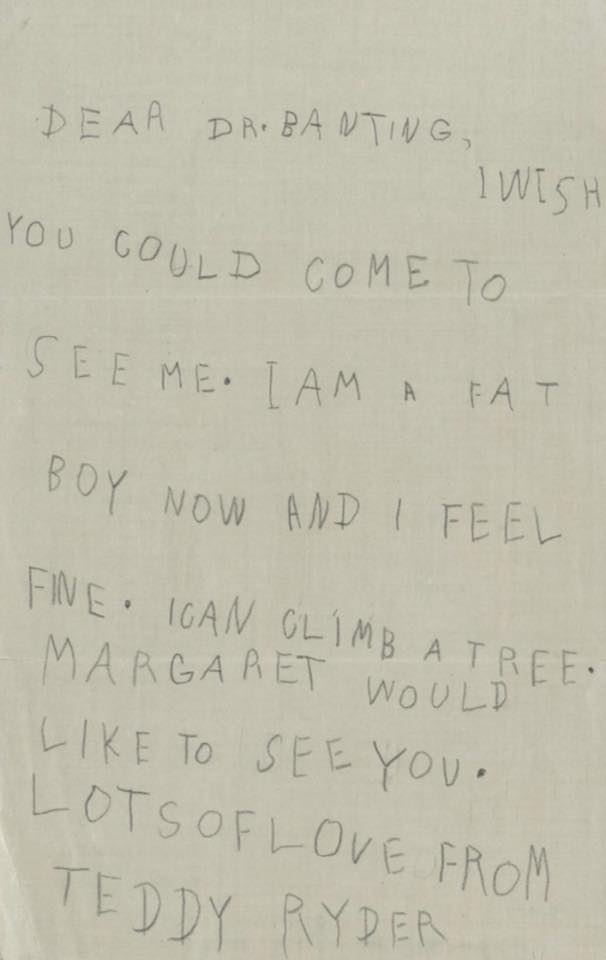
Meet Teddy Ryder, one of the first kids to ever receive insulin. When he went to Dr. Banting in 1922, he was 5 years old and only 26 pounds. Pre-insulin T1D treatment was essentially a starvation diet that ended in death 100% of the time. Within days of taking insulin, Teddy began gaining weight. This letter you see is a letter 6-year-old Teddy wrote to Dr. Banting after he’d been on insulin therapy for a while. It reads “Dear Dr. Banting, I wish you could come to see me. I am a fat boy now and I feel fine. I can climb a tree….Lots of love from Teddy Ryder.” Teddy lived until he was 76, thanks to Dr. Banting and the discovery of insulin.
Extreme unintentional weight loss can be a symptom of T1D. I personally lost about 19% of my bodyweight in about 2.5 weeks before I was diagnosed, and just like Teddy, I quickly regained it upon starting insulin. When I was admitted to the ICU, my BG was 965 mg/dL. It’s supposed to be around 80 mg/dL. I’m extremely fortunate that I was not in a coma. There isn’t an exact number that comas occur, but comas have been reported in some T1Ds starting around 750 mg/dL.
Unlike the kids in this hospital ward, I was lucky enough to start insulin almost immediately after diagnosis. In ICU I received mainly IV insulin, so it was 3 days post-diagnosis before I had my first insulin shot. I have no memory of my first insulin shot. However, I will never forget the first time I gave myself an insulin shot. It’s the most vivid memory I have to date.
------------
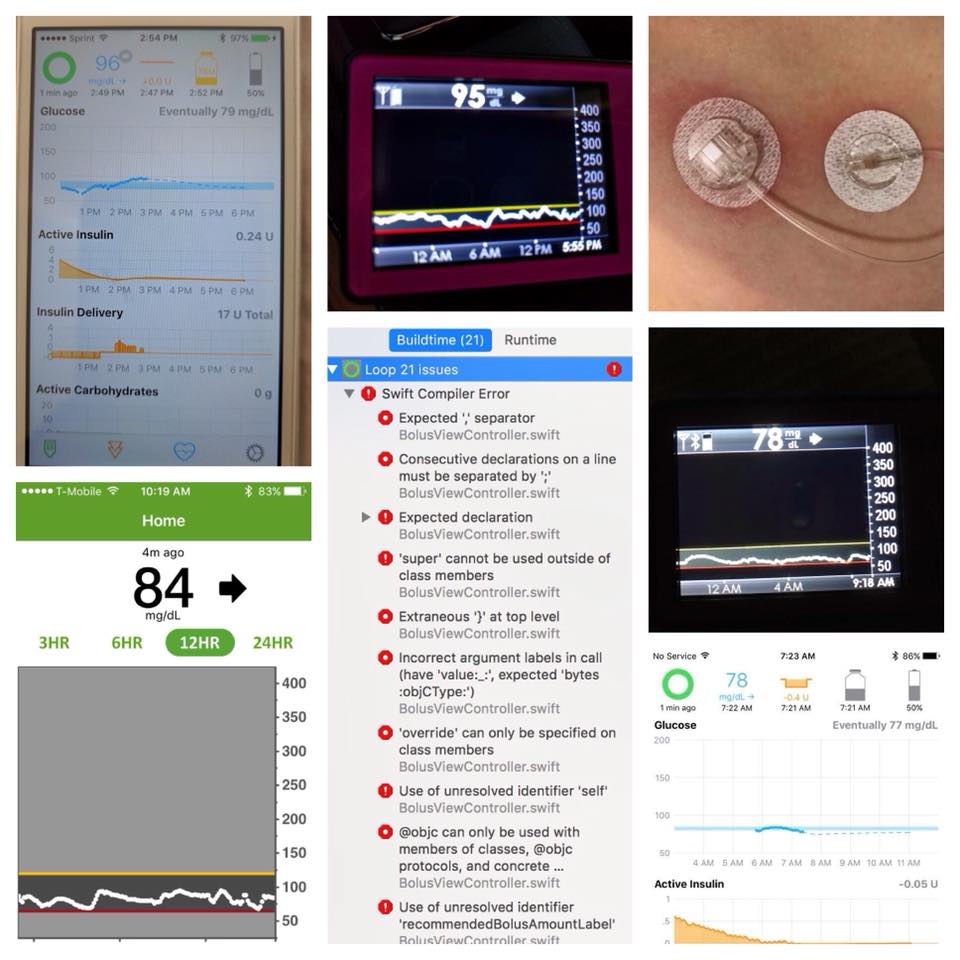
On February 27th this past year I became an Apple Developer in order to build myself an artificial pancreas called Loop. It’s something I never would have imagined I’d actually do, and the knowledge and satisfaction I gained from the process is yet another silver lining of T1D.
Though I wanted Loop for quite a while before I actually built it, the caveat is it is not for sale and never will be. If you want it, you build it. Period. I’ll admit, this was extremely daunting given I don’t have a technical background. With all of my other T1D technology, I like having Customer Support just a phone call away. If something breaks with Loop, well, I have to troubleshoot it myself. This was an exciting and scary challenge at the same time. I actually spent 6 months learning about Loop before I even attempted the build. I also got incredible support from other T1s and T1 parents who had already built Loop and from a detailed online guide (https://loopkit.github.io/loopdocs/).
When I actually dove into the build process, I was overwhelmed with the number of errors I had. Yet when I worked through each one and eventually had a functioning artificial pancreas as a result, I felt a kind of pride that is hard to verbalize. It was way more satisfying than downloading an artificial pancreas app ever would be.
Loop is essentially an automated insulin delivery system that is part of the #WeAreNotWaiting movement, meaning T1Ds deserve better technology than is commercially available. Without question, Loop is superior to any system available for sale. Loop and other DIY artificial pancreas systems are the ONLY systems currently available that allow T1s to achieve non-T1 results. (HUGE shoutout to Nate, Chris, Ben, Dana, Scott, Katie and anyone else I missed in making Loop what it is today!) Though Medtronic has an artificial pancreas on the market, the lower range is 120, which is 40 higher than I strive for.
As you know from previous posts, I am not currently on Loop. While I definitely do think at some point in time I’ll resume Looping, I needed a break from wearing a pump. I am also allergic to pump site tape (yes I’ve tried Skin Tac, barrier wipes, you name it!), so that was part of my decision too.
For those of you new to artificial pancreases, I want to clarify that while it does make many aspects of T1D life easier, it still needs human input to operate. You tell Loop when you eat, what you eat, when you exercise, etc. And you still have to wear/carry the hardware it requires. Pump site issues can also still happen, and no algorithm can regulate BGs if the insulin isn’t entering the body in the first place. So, in theory, while an artificial pancreas may sound perfect, it’s still far from a cure.
------------
Thank goodness for technological advances!
------------
For today’s #T1DAwarenessMonth post, I’m sharing a T1 parent’s perspective:
“Yes you could. And you would.
You would sit in that hospital bed, wrapped around your child in vain, too late to protect them but unable to stop trying. You would listen intently to things you absolutely don’t want to hear, but you have to.
Subcutaneous. Insulin. For life. Synthetic hormone. Auto-immune. No cure. Carbohydrates. Ketoacidosis. Glucagon. Coma. Brain swelling. Ketones.
You would stare at the needles as they bring them to your child. You would remember how hard they cried after immunizations, and your mind would recoil away from the reality of how fractional that is now. You would hate the nurse who debates with your terrified child about the shots that will not stop coming. Ever. Logically she’s saving her, of course, but instinct says she’s hurting your baby.
You would do it all. Because the luxury of choice is gone.
You would wake up every two hours in a panic to stab them again to know if they’re ok. You’d drag your wailing, weeping 3-year-old out from underneath the kitchen table and grimly hold them down for the third shot of the day. You’d wish for your own death at that moment, but you’d do it. And again. And again.
Eventually they do stop crying, the nurses were right about that. Somehow that point is a fresh level of hell, but you still keep going. It gets easier, but this stage never leaves your heart and mind.
The response is one made with good intentions. I know people mean to express their sympathy, their horror. I know it’s hard to wrap your mind around it, we had a hard time, too. I get it. Just understand what goes through our minds every time this is said is the crushing trauma of learning we would have no choice but to do this.”
------------

Growing up in St. Louis, it felt like everyone just knew I had T1D. I’m sure that’s not the case, but nor do I recall ever telling anyone directly. My T1D walk was, after all, an annual school-wide community service opportunity, and I got special permission to inject in the classroom after my mom helped reverse a policy that was causing me to miss way too much instruction-time in the nurse’s office to care for my T1. So, to some extent, it felt like everyone just knew.
Fast-forward to college, where I went 1,218 miles from home and didn’t know a single person. And no one then, of course, knew I had T1D. College was the first time I ever really felt different because of my T1D. Not different in a bad way, just different in a well, different way. This picture you see here is from a pool party freshman year. I went to college in Miami, whereas I’m sure you can imagine pool parties were abundant. But let’s face it: if I kept my cover up on and didn’t fully participate, I’d be different. If I went straight in to the foam party with my pump and CGM on, I’d be different. And there’s no way I’d decide to do the former because of my pump and CGM, but this really was the first time this realization crossed my mind. T1D is nothing to be ashamed of, and being different is not a bad thing. That’s the mentality I had as freshman-me and that’s the mentality I still hold today.
In almost all circumstances, I don’t hide my T1D, though there are a couple I can think of. That said, I also try to be as respectful as possible around people unfamiliar or uncomfortable with needles. If I have a relatively easy option of stepping aside to inject, I without question choose that over injecting right in front of everyone. Or oftentimes I’ll do everything in my lap beneath the table if I’m out to eat, for example. Legally, however, the Americans with Disabilities Act does grant T1Ds the legal right to inject in public. And that’s really, really important.
That said, stares, comments and questions definitely still happen. I never, ever mind a genuine question or opportunity to educate someone about T1. Luckily, in about 99% of cases, the person means well and is just curious. The other 1% is somehow much more memorable. At 24, I can handle whatever response comes my way. It’s the little T1s I wish never had to witness this 1%.
------------
Today’s #T1DAwarenessMonth post is on T1D and eating disorders. 40% of T1D girls and women have or will develop an eating disorder. Thankfully, I don’t have personal experience with an eating disorder, but T1D certainly has permanently altered my relationship with food. Let me try to explain.
As you saw in a previous post, insulin can be life threatening with the slightest imprecision. A huge variable in calculating the correct amount of insulin is knowing the accurate nutritional profile of what you are eating. When your life depends on knowledge of nutrition facts, it becomes super easy to overanalyze food. I’ve had to track every single bite of food since I was diagnosed with T1D. Years ago I had to use a paper logbook, but thankfully there are easy-to-use apps now.
There’s also a concept T1Ds call pre-bolusing. Basically, this means injecting insulin 15-20 minutes before eating because synthetic insulin is much slower than the insulin a normal pancreas produces. In short, this means I need to know how much I’m going to consume during a meal 15-20 minutes before I actually start eating, and oftentimes even before I’ve seen the food. If I’ve already injected for the food, I have to finish everything I dosed for, whether I want to or not.
For me, T1D can also cause some anxiety in food situations. For example, how am I supposed to pre-bolus at a restaurant when I have no clue when the food will come? What if I’ve already pre-bolused and I have to send my food back for some reason? (It can be very dangerous to pre-bolus too early). How do I know what ingredients are actually in my food to dose appropriately? How do I know how large the portion will be? Even if I’m eating something out of a package, nutrition facts can be off 20% in either direction and still comply with FDA guidelines. This 20%, however, makes a big, BIG difference for a T1 calculating their insulin dose largely off of the facts.
Moreover, I often have to eat when I don’t want to because of hypoglycemia (low blood sugar). Sometimes it’s right after a huge meal or in the middle of the night. Nothing about eating in these situations is normal.
I also don’t produce amylin, which is a hormone healthy pancreases produce that plays a role in digestion and suppresses appetite as you eat. If I wanted this satiety feeling, I could inject synthetic amylin when I eat, but given it’s not vital for survival, I choose not to.
Finally, insulin has a strong correlation to my weight. If I accidentally take too much (because always taking the perfect amount is impossible), I gain weight. From all of these reasons and others not listed, I hope you can see why T1D can easily distort a normal relationship with food.
This article details diabulimia, a T1D-exclusive eating disorder. To summarize, extremely fast weight loss is possible by giving too little insulin. It’s extremely dangerous and unfortunately common among T1s.
------------
Today’s #T1DAwarenessMonth post is the misdiagnosis of T1D, which is far too commonly diagnosed too late. The saddest part is that with an earlier diagnosis, these T1s could have lived long, healthy, happy and normal lives with T1. Many of them had even been to the doctor and received a wrong diagnosis.
Every few months, the T1 community’s heart breaks upon learning of a newly diagnosed T1’s passing. One particular T1 named Kycie pulled the heartstrings of the T1 community perhaps more than ever before. In 2015 she passed away at just 5 years old after going into a coma from undiagnosed T1D.
This 15-minute video shares Kycie’s story and touches upon T1D misdiagnosis more broadly too.
------------
Today’s #T1DAwarenessMonth post is to answer a question I received earlier this week: “I had no clue T1D was so encompassing/consuming and required so much patient responsibility, but I’m curious, how does T1D make you feel physically on a day-to-day basis?” Here’s the good news: the overwhelming majority of the time I feel absolutely fine with T1D. In fact, I think in my whole life I’ve only ever taken 2 sick days from school/work due to T1D. The hard work I put into T1D management pays off in how I feel, so there’s definitely strong incentive to maintain tight control.
The CGM graph pictured is from Thanksgiving yesterday, where I ate 2 huge meals. (I’m in CST and it’s set to PST still, so it was taken about 2.5 hours after dinner.) As a refresher, I try to stay within the lines all times, though that is impossible. Not feeling well because of T1D typically only occurs when I am outside of the lines, or quickly changing within range.
Symptoms definitely vary among T1Ds, so I’ll share some basic ones.
When I’m below range (or in other words, hypoglycemic), I start shaking and sweating. I become extremely hungry, weak, faint and oftentimes anxious. Lights and sounds start to bother me (i.e. it can be painful to listen to music when I’m low). It feels like there are bees in my mouth, and sometimes it feels like I no longer have a tongue. If I try to stand, my legs feel like Jello. If I’m extremely low, which thankfully is quite rare, it becomes extremely difficult/impossible to talk/make any noise and eat.
If I’m above range, I also get very hungry, but also thirsty. I often have a pounding headache and queasiness. I feel sluggish and irritable. Most adult T1Ds describe being above range in line with what it feels like to be hungover.
The past few years I’ve definitely developed some glycemic unawareness, meaning I don’t experience many symptoms until I’m seriously out of range. While this is good in the sense that I feel much better on a day-to-day basis with T1D, it’s actually a really bad thing that I no longer experience the “warning signs” my body should produce to let me know something is wrong. Testing frequently is therefore extra important for me.
When I feel sick from T1D, the main reason is due to other health conditions and medications that make staying in range incredibly difficult/impossible, and thus I experience the symptoms described above. All in all though, I’m extremely thankful that T1D really doesn’t make me feel sick too often, and typically when it does, I can get back in range quickly and the symptoms also disappear.
------------
Today’s #T1DAwarenessMonth post is on glucagon, which is a life-saving emergency injection I always carry around in case I’m ever found unconscious due to a low blood sugar. Essentially, glucagon prompts the liver to release glycogen stores. Thankfully to date no one has ever had to use glucagon on me. That said, with T1D, anything can happen, despite extreme diligence and conscientiousness in T1D care. Whenever I come across a story where glucagon saved a T1’s life, or a T1’s life may have been saved had someone used glucagon, I always vow that I’ll do a better job teaching those around me about glucagon. But it can be hard.
Let’s face it, glucagon is a huge responsibility. Teaching someone who has absolutely no experience with T1D or needles whatsoever when to use glucagon, how to draw up the hormone and how to inject it is extremely intimidating. In a perfect world I’d say just call 911 if a T1 is found unconscious (like hopefully you’d do anyway!), but in reality, every second really does matter. And to add to the complexity, of course there are reasons aside from low blood sugar that a T1 can lose consciousness.
Moreover, when to tell someone about glucagon can feel like a big decision. In theory I’d like to teach everyone I spend any time around the basics, but it can be a lot of personal information to share too soon, or in special situations, such as professional settings. I’ve therefore taught the people I spend most of my time with how to use glucagon, and then I wear a medical ID bracelet 24/7 that would hopefully expedite glucagon administration by paramedics given they’re all trained.
Just like CPR, I consider knowing how to use glucagon a really valuable life skill. It’s needed much more commonly than you might think, and T1 is much more prevalent than you might think. Whether you know it or not, there’s a good chance you probably know/know of at least 10 T1Ds in real life. So, if you have any interest in learning, please watch this video or ask me for an in-person demonstration. You never know when you might save a life!
------------
For today's #T1DAwarenessMonth post, I'm sharing a story a T1 mom posted about her daughter's experience receiving glucagon earlier this week. I'm so glad she's okay, and I'm thankful they were willing to share the story to help spread awareness.

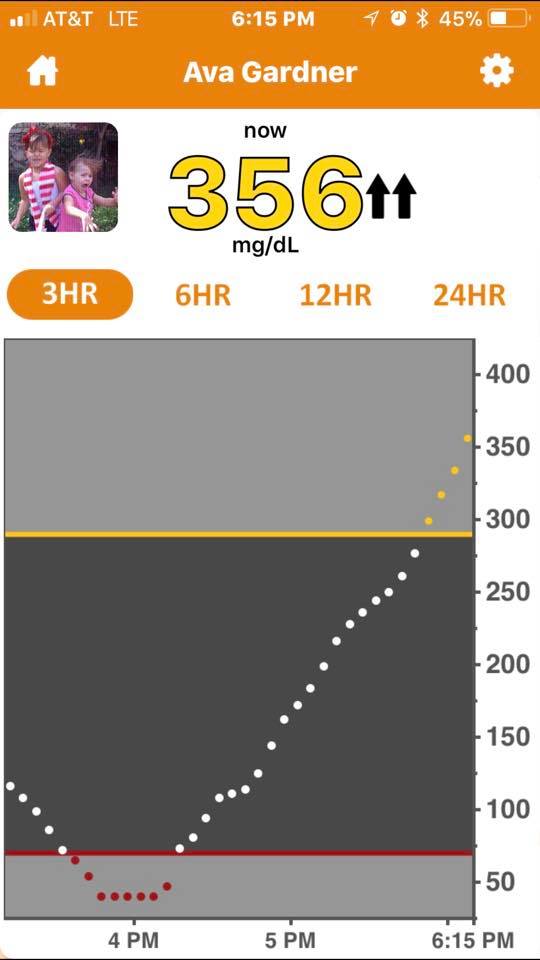

“We had a major medical emergency this afternoon in Applehill!! In an instant things went from a laughing happy go lucky time to a serious scary scene. Ava could have very easily died this afternoon. I am trying to wrap my brain around that. It was so fast. Never have we seen such a fast low!
We were taking pictures. She mentioned she was low. I checked and she was 65 one arrow straight down. Ethan ran off to the car to grab some sugar to treat her. Within 2 minutes she was acting strange. Legs buckling, laughing uncontrollably, wandering around. I asked if she was okay and she said she felt really strange. I walked over to help her move to a place to sit and she got extremely combative very fast. Pushed me away, told me to leave her alone. She ran off and tripped and face planted. Got up and tried to run away from me again, ran straight for a flight of stairs. I yelled for the big girls to get their dad!!!
We all realized in that moment things had gotten critical. I grabbed her from behind as her knees kept bucking and her arms were convulsing and tried to sit her, and she was so combative that we both rolled almost completely over and a backwards roll (in the mud).
We continued to fight, (she is soooo strong), her big sisters held her down, we attempted to put sugar in her mouth and she refused. Attempted to give her juice and no. We fought for a few minutes and she passed out and started to convulse again.
Ethan ran to get the glucagon shot came back and we switched as I was physically exhausted from fighting her (her flight and fright was in full force). During this time she passed out a few times and then would come back.
We flipped her over and I gave her the shot.
Then we called 911 as she passed out and convulsed a few more times.
Paramedics got there about 10 minutes after her glucagon shot. And although she got up and physically walked over to a park bench and was talking she does not remember any of it.
They tested her and she was 40. This was 10 minutes after her shot.
They gave her 2 glucogel packs 15-20 minutes apart and finally she was up to 75 and able to leave.
Both her and I were coated with mud (her more than me).
She was extremely embarrassed for the lack of control this whole episode gave her. I am horrified that this could happen to her some day without loved ones around to help.
I pray that others show her compassion when she has an altered personality and know that is her horrific disease that she has zero control over.
I pray that she always has enough supplies and others around are educated enough to see the warning signs of an impending emergency.
I am truly mentally drained and feel so sick to my stomach over what we all just went through. Terrifying. And of course now she has to deal with the rebound horrible high. My poor baby girl.
But my biggest prayer is for a cure. A damn cure for this damn disease!!! Type 1 diabetes you freaking suck!!!”
------------

Today’s #T1DAwarenessMonthPost is on diabetes camp. Yes, you read that correctly: there are entire camps devoted to children with diabetes. They are truly amazing places, and I went to two different ones as a camper, CIT and counselor. One was a traditional summer sleepaway camp and one was a camp on a cruise ship. The picture above was from my first year as a counselor with a few of my 8 year old campers.
So what makes diabetes camp so special? For many kids, camp is the first time they meet another T1, or at least a T1 their own age. T1D can feel extremely isolating for kids, and knowing someone else your age going through the same thing can make a world of difference. Before camp, the only T1s I knew were my great aunt and my mom’s cousin who is 20 years older than me, so it was really special meeting other T1 kids. Diabetes camp is also a place where “firsts” are celebrated. First shot by yourself. First pump site change by yourself, etc. For kids (and their parents), these “firsts” make a big, BIG difference. They make some degree of independence much more possible (i.e. birthday parties, playdates, school trips etc.). Nurses still took care of overnight T1D care at camp, and most T1 kids can sleep through needles and shots entirely (I can’t!).
------------
Today’s #T1DAwarenessMonth post is on the name of type 1 diabetes, which actually has quite an interesting history and is fairly controversial. According to a study, 80% of Americans can’t distinguish between type 1 and type 2 diabetes, and 36% percent think there are type 3 and type 4 diabetes too.* T1D has been called many names over the years, including insulin-dependent diabetes, juvenile diabetes and childhood onset diabetes. Currently, there’s a petition out to rename T1D again. (And I actually know the amazing creator of the petition in real life - Jamie Perez)! She explains the reasoning better than I ever could, so if you’re interested in this issue, I encourage you to read the linked petition.
Personally, I strongly support a new name for T1D because since “diabetes” in general is so well known — yet T1D causes and management commonly have nothing to do with what the average person thinks of diabetes — it causes an abundance of misconceptions, stereotypes and stigmas for T1Ds. As an autoimmune disease, T1D falls into the same category of diseases such as multiple sclerosis, rheumatoid arthritis, celiac, hashimoto’s, lupus and many others, but how people perceive other autoimmunes versus diabetes is like night and day. I’ve never had rude comments, condescending remarks or jokes about my other autoimmunes, yet with diabetes, I hear it all the time. More importantly, however, lives are lost when people assume they can’t have diabetes since they are skinny, eat healthy, exercise daily, etc., yet little do they know T1D has nothing to do with any of that. In short, I think a name other than T1D would truly save lives and make life easier for T1Ds.
Petition: https://www.change.org/p/revise-names-of-type-1-2-diabetes-to-reflect-the-nature-of-each-disease
*Source: Medtronic D-awareness study, 2007.
------------
Today’s #T1DAwarenessMonth post is on T1D cure research. I’m incredibly optimistic about the work of Dr. Denise Faustman. She runs The Faustman Lab at Massachusetts General Hospital and is already in Phase II of human trials. Amazingly, she’s repurposing the BCG vaccine for the reversal of T1D. (The BCG vaccine is commonly used in countries with high prevalence of tuberculosis to prevent TB). Whereas lots of research focuses on newly diagnosed T1Ds where the autoimmune attack is still in progress, she is focusing on long-term T1Ds — just like me — where the pancreas killed itself 10+ years ago. She saw positive results from her Phase I human trials. I’d bet money that she’s the one who will find the cure.
That said, I’m also incredibly optimistic about stem cells. There’s a company in San Diego called ViaCyte that I currently view as the leader in the T1D stem cell space. I’m excited to see what progress they’ll make in the coming years.
The Juvenile Diabetes Research Foundation (JDRF) and the American Diabetes Association (ADA) are two other well-known players in the T1D research space. Many of their projects focus on improving quality of life for T1Ds and making T1D management easier. While still important, I’d prefer my personal donations to go to an entirely cure-centric organization since I’m 100% fine managing my T1D as is until a cure is found. The majority of the ADA’s research budget goes towards type 2 diabetes, so I also prefer to support T1-specific organizations given T1 cure research has nothing to do with type 2 diabetes.
While of course I hope a cure is found, I never think of what it would be like living T1D-free since there’s no point in getting my hopes up. I’ll be thrilled if I see a cure in my lifetime. Realistically, I think a cure is still decades away from being commercially available, as politics and regulations definitely slow down progress, even though I believe from a scientific standpoint a cure is close.
------------
Another month, another pumpkin. And just like that, today marks the final day of #T1DAwarenessMonth. Thanks so much to everyone who took a moment over the past month to read my posts, like them, and share them. I’m so grateful for all of the messages and encouraging words I’ve received.
Awareness posts can get annoying. I get it. I really do. But #T1DAwareness is so important because everyone thinks they know what diabetes is, even if they can’t tell you the difference between type 1 and type 2. False misconceptions are often even more dangerous than pure lack of awareness in the first place.
So first off, I hope my posts gave you a glimpse into the reality of life with T1D.
I hope they surprised you and made you aware how little we often know about what someone else is going through, health-related or not.
I hope you realized that T1D has no “look.” It can be a baby still in diapers to a senior heading off to college to a mom of 4 kids to an Olympian athlete. No one is too young (or too old) to get T1D, and nor does anyone outgrow it.
I hope you learned that T1D and what the common person knows of “diabetes” are two entirely different diseases. T1D is a non-preventable autoimmune disease and has nothing to do with lifestyle choices, such as diet and exercise, or obesity.
I hope my posts encouraged you to stop cracking diabetes jokes and using diabetes hashtags.
Living with a stereotyped, stigmatized disease is not fun, whether you have type 1 or type 2.
I hope you are familiar with T1D’s symptoms and common false diagnoses. “It’s the flu. It’s a virus. It’s strep. It’s a UTI. It’s just a growth spurt.” For your sake, I really hope it is, but please, do yourself a favor and rule out T1D with a quick, simple blood test.
But most importantly, I hope you learned something that might save a life one day.
My T1D posts will end until next awareness month, but T1D will, of course, continue humming in the background of my personal and professional life every minute of every day. It has played such a pivotal role in shaping my life and character, and as cliche as it sounds, it’s a large reason I am who I am today. And for that I’m thankful.


New comments are not allowed.